








Don’t worry, I haven’t suddenly turned into a conspiracy theorist 😉 . I’m talking about a new systematic review which appeared in the May issue of Archives of Disease in Childhood. It identifies head-covering during sleep as a major risk factor for SIDS.
While the article notes that bedsharing babies who die of SIDS are less likely to be found dead with their head covered, another review of some of the literature published by some of the same research team members last month in Pediatrics points out (emphasis mine):
In the New Zealand study but not GeSID, bed sharing was associated with a decreased risk for being found with the head covered. Head covering during co-sleeping is common. Baddock et al reported that there were 102 head-covering episodes for the 22 infants studied. The majority of head covering during co-sleeping was by inadvertent movements by the adults as they changed position during sleep. Sixty-eight percent of head uncovering was facilitated by the mother, and half of these events were prompted by the infant. It is possible that for SIDS cases, when mothers wake up, they uncover the infant’s head. They then discover that the infant has died, thus reporting the low incidence of head covering while bed sharing.
The three Baddock et al studies from New Zealand, are a very interesting read. Each examines a certain aspect of an experiment comparing 40 bedsharing mother-infant pairs vs. 40 cot-sleeping (cot being non-American English for crib) ones over two nights. While I wish I could tell you the conclusions from these studies coalesce into one big “A-ha!”, they don’t. The information gleaned from them is, nevertheless, quite valuable in providing some more puzzle pieces, so to speak, and will probably serve as an important basis and experimental model for future research.
The first study, Bed-sharing and the infant’s thermal environment in the home setting, describes the experiment’s setup: The 80 babies, all born at term and aged 0-6 months, were attached to various monitors recording heartbeat, blood oxygen saturation, body (rectal and shin) temperature, respiratory pattern and air quality around the infant’s nose, and electrocardiogram. The babies and their mothers/parents were also recorded by video all night long. 40 of those babies shared a bed with their parents, all of whom expressed ideological reasons for doing so rather than ‘reactive bedsharing’. The other 40 were kept in cots in the parents’ bedroom.
The main conclusion of this particular study was that bedsharing infants tend to sleep in a warmer environment than cot sleepers, but they tolerate this well and do not overheat. However, I found table 5 in the study to be most informative (click on the thumbnail to see a screenshot of the table):
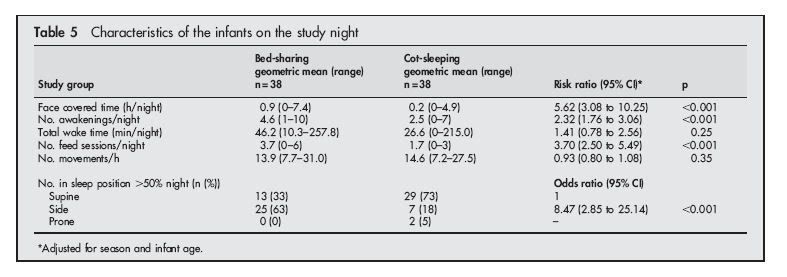
Bedsharing infants had their faces covered for X5.62 the time period that the cot-sleeping babies did. They also woke up more often, fed more frequently during the night and were awake for a longer period of time (though this last prameter was not statistically significant).
The second study, Differences in Infant and Parent Behaviors During Routine Bed Sharing Compared With Cot Sleeping in the Home Setting, also elaborates upon this in the abstract:
Head covering above the eyes occurred in 22 bed-sharing infants and 1 cot-sleeping infant. Five of these bed-sharing infants were head covered at final waking time, but the cot-sleeping infant was not.
The study further divulges that most of the covering happened as a result of the parents shifting in bed. Uncovering was usually performed by the mother; most often, the impetus for this was the baby’s movements (see Table 4).
There is also a discussion regarding the fact (also seen in Table 5 of the first study) that most of the bedsharing infants spent the large part of the night in the side-lying position, rather than the recommended supine position, as do most of the cot-sleepers. Baddock et al tend to think that side-sleeping might not be as dangerous for bedsharers as compared to non-bedsharing babies, as the typical mother-infant bedsharing position tends to prevent the baby rolling from side to prone sleeping. However, one infant out of 23 side-sleepers in this study did, in fact, roll into the prone position during the night.
The third study, Sleep Arrangements and Behavior of Bed-Sharing Families in the Home Setting, focuses on the bedsharing arm of the experiment, consisting of 40 bedsharing infants and mothers. We learn that the mothers are predominantly of Anglo-Saxon origin, most are highly educated, and all breastfed. 3 out of the 40 mothers (7.5%) smoked, despite the admonition not to bedshare if one smokes. None of the mothers drank alcohol to excess.
Some more interesting tidbits:
1) In most cases of bedsharing, fathers were absent. (Do fathers count in the “family” part of the “family bed”? Doesn’t seem like it.)
2) In 2 of the 4 instances the bed was shared by siblings, a sibling spent time sleeping next to the baby – also a no-no according to safe cosleepng rules.
I was intrigued that despite the fact that various measurements of the infants’ physiological states (pulse oximetry, ECG, carbin dioxide levels around the babies’ noses) were ,obviously, painstakingly gathered, none were provided except for the thermal measurements and an offhand reference to “no oxygen desaturation events <90% with head covered (data not given) …was observed” in the second study. So I contacted Dr. Baddock via email asking her about this, and she was kind enough to respond with the following (emphasis mine):
I have previously presented to the International SIDS Conference an
analysis of episodes during the night when the inspired CO2 was elevated
to at least 3%. Analysis of 80 of these events showed they were
associated with an increase in the frequency of breathing and that
oxygen saturation was maintained. In the majority of events the increase
in CO2 was associated with covering of the face. The 80 events were from
22 bedshare infants and one cot sleep infant. Our suggestion is that
normal healthy infants maintain oxygen saturation when the head is
covered through increasing ventilation but we hypothesize that infants
with impaired cardiorespiratory control may not do this successfully.While desaturation below 90% was recorded on many occasions during the
night, the level of CO2 for the preceding 30 seconds was seldom above
1%. I have not linked these events specifically to the time scale on the
video, but the low CO2 values would suggest these desaturations were not
associated with head covering. They were preceded by central apnea and
were twice as common in bedshare infants.
The episodes of central apnea more common iin bedsharing infants look like McKenna’s findings from 1998; it would be interesting to know if the apneas precipitated other physiological events such as bradycardia, and how long the episodes were.
Those “infants with impaired cardiorespiratory control” who may have trouble responding to a respiratory challenge such as head covering seems to jive with the recently-popularized SIDS/serotonin theory (emphasis mine):
Researchers examined brain tissue from SIDS victims and found that their serotonin receptor binding was lower than normal in the brain stem, an area that helps control vital functions like breathing.
More recently scientists found that SIDS cases were more likely to have a certain variation of a gene that produces the serotonin transporter. This cell component can pump the serotonin back into the brain cell to mute the messaging process. The researchers suspect that people with the variation harbor more effective transporters than other people. Preliminary examinations of brain stem tissue also suggest that some SIDS victims have an excess of these more effective serotonin transporters.
Together these results could mean that the serotonin communication system in some infants does not work properly, perhaps sending out fewer messages than normal. Possibly the faulty system prevents children from responding to life-threatening events during sleep, such as increased levels of carbon dioxide, a harmful waste product eliminated by the lungs during breathing. Babies can experience excessive levels of the gas when they rebreathe air trapped in bedding, for instance. Normally, the serotonin system may help sense the problem and trigger mechanisms that increase breathing to expel the carbon dioxide.
Animal research supports this idea. For example, scientists discovered that normally an increase in carbon dioxide strongly stimulates cells that contain serotonin in the brain stem. Also early evidence indicates that a drug used for depression, which inhibits the transporter’s activities and increases messaging in the serotonin system, enhances the response of rats to carbon dioxide. In ongoing research, scientists also find that they can decrease an animal’s response to carbon dioxide by killing cells that contain serotonin in the brain stem. In addition, mice bred to lack most of their serotonin cells have abnormal breathing and some die during infancy.
So there you go…no definite conclusions, but these seem to me to be some very few pieces of the great puzzle that SIDS/SUDI currently is that can be put together : A respiratory challenge such as head covering or prone sleeping (though by no means exclusive to those two mechanisms!) to an infant who is, due to a biochemical brain imbalance, unable to respond sufficiently to clear his airway. This would help to explain why small babies who bedshare are at risk for SIDS/SUDI, even if precautions are taken. And also that even “ideological” bedsharing parents are not completely immune to dangerous cosleeping…
 :
:  :
:  :
:  :
:  :
:  :
:  :
:  :
:  :
:  :
:  :
: 
Filed under: Infant sleep |

So you haven’t turned into a conspiracy therorist…Too bad I think you would be most entertaining as a conspiracy theroist….Not that you are not entertaining now.
I was wondering if you were going to address the serotonin thing. I just read about it in the newspaper recently. I think it would be great if they could test babies to see if they are likely to have a serotonin problem so that they can be watched more carefully. However, I’d imagine most NP advocates wouldn’t allow the tests anyway.
You sure do have a keen interest in bed-sharing. I’m just really unclear why because I doubt you ever did it, at least successfully. It sounds like you are discovering the basics behind the Diathesis-stress model. I am waiting for you to look into how many children expire for unknown reasons inside the boundaries of a safety approved crib. Why would a child, sleeping exactly where the crib industry wants it to (their product), die? Well, many empirical parents who don’t believe that lifesaving decisions for their child are best made by a corporation who, via a huge conflict of interest, sells a product that does kill kids. Parents are getting sick of the real “cover-up” and will continue safely sleeping next to their child. Visit http://www.co-sleepingsurvey.com to view over 7600 parents from around the world who do co-sleep and bed-share safely, and will maintain no matter how many “correlational” studies are manufactured in an effort to sell more cribs. Point is, in line with the diathesis stress model, only the bed-sharing parent remains with their child to negate any possible night time stressors such as head covering with blankets. Regardless of the 22 mother-baby pairs that were referenced, shared sleep remains scientifically safer. The child that sleeps alone will only receive cursory attention at best, and none when a parent is sleeping somewhere else. Why would the AAP recommend room sharing????? After years of promoting the nursery, doesn’t this seem odd? Undeniably children who sleep in a separate space will not be saved from positional asphyxiations, choking (acid reflux), SIDS, crib defects, abductions, fires, etc.
And you, as a “mainstream parent” and a “family physician”, will keep your head down, and not blog about those deaths. Presumably because you would rather blame and point your finger at a parent that considers themselves more “attached” to their child than you were to yours. Stop lying to yourself and ask your beloved crib industry for some stats on that.
It never ceases to amaze me that NPers will resort to childish personal attacks like ” I’m just really unclear why because I doubt you ever did it, at least successfully.”
Really? She is really a closeted “failed” co-sleeper. Obviously, you haven’t read the many posts here about co-sleeping and the safe methods this blogger proposes.
Clearly, you feel that it is a personal attack on you to discuss these matters. Maybe you should look at why others who voice opinions and discuss research upset you so much. Everything is not a conspiracy try as you might to make it so.
Hugh, you’ve read and commented on my posts regarding this issue before. If you’ve understood them, you know very well that these things have been studied, and bedsharing in very young or small babies is a risk for SUDI/SIDS/suffocation. A bunch of self-selected, ideological cosleepers answering an online survey and all protesting “Of course we follow all the rules all the time! Honest Injun!” doesn’t make for a very reliable scientific study of the subject…it just seems like they doth protest too much.
As pointed out, in some cases, not only the bedsharing parents sleep in the bed with the baby, and some of the mothers even smoked, which is a known risk factor for bedsharing.
I’m not aware that the AAP ever recommended separate nurseries for small babies – in fact, until their most recent policy statement in 2005, they didn’t make a blanket recommendation not to share a bed with the baby, just that under certain conditions, it may be hazardous ( compare to the 2000 policy statement). I also think that crying “conspiracy” every time the research doesn’t go your way is further proof that though you NPers like to pretend your methods are science based, you really couldn’t give a flying fart what the science says, even if your ways are proven harmful. So knock it off with the false appeals to science already.
Incidentally, I have no ties, financial or otherwise, with any crib manufacturers, formula companies, whatever. I have roomshared with all 3 of my kids until 6-8 months (my eldest initially slept in his baby carriage next to my bed, then we got a bassinet with mesh sides which served him and my other two). In fact, most parents I know roomshare in the first few months – “mainstream” or otherwise but I can’t see any of us making claims of being more “attached” to our children as a result.
Oh, and yes, I am quite familiar with the diathesis-stress model (because I really am a family physician, no need for scare quotes) …the whole idea behind the discouragement of sharing a sleeping surface with one’s infant is to help lessen the stress part of the equasion. How is this a problem?
whoa, that is a LOT of head covering! and do the co-sleeping parents just think this is normal? they just uncover the baby and go back to sleep???
wow, i’m floored. i co-slept with my daughter like i’ve said, and one time i woke up with the blanket up on her face (not over, at mid-face level). i freaked out! after that, i made up the bed so the blankets only came up to my chest. DD’s head was well above that (usually way up by my face. we had no headboard and i don’t use a pillow, so i thought that’d be the safest). i didn’t want to take any chances of that happening again.
i don’t understand… don’t other people think it’s not cool if the covers go over the baby’s head?
Hi Estherar,
I don’t want to seem “attacking” but, you do write very negative, and scientifically spun posts. So, naturally, I would have a response, or “attack” as you might see it. If you write something that was neutral, or unbiased, you would not hear from me…I promise.
Your personal experience with your children does not include knowing how to bed-share, so why would this be something you are sure other people should not do? What was your reasoning for not bed-sharing? Was it your own and if so, are you sure it was your own instinctual process that led you to purchase crib devices to help you? If you think you are not tied to cribs and their sale, well you are wrong. Maybe you did listen to someone who told you not to do it. Maybe their ads got to you, or your parents and then you never thought for yourself… Either way, you have no experience so how is your information worthy? If you are just another person interpreting research then…aren’t you doing it from the perspective of a non-co-sleeping parent? Doesn’t it seem a little wrong that you would be commenting on the impossibility of something you yourself have not done? I mean, it would be like me telling you how to be a doctor.
As for discrediting the 7600 families who have no reason to lie about…by saying that they all must just be lying. That is juvenile, and does not relay any “professionalism”. Are you saying that 7600 people sought out a public forum to cover up killing their child? Nice. Sure there was no one presiding in a lab coat, or working out some senior year credits, but the parents do have experience doing it. They were not paid in anyway, and their responses were and continue to be generated by ridiculous information like what you purvey (thanks). Are you saying that they just got lucky? And, 7600, yes that could be seen as small…but when the number reaches 50,000…will it still just be a bunch of “honest injuns”? That is not only a classically ignorant statement but a racist one as well.
And your comment….”the whole idea behind the discouragement of sharing a sleeping surface with one’s infant is to help lessen the stress part of the equation. How is this a problem?”
Well, it’s a problem because there is science that you choose not to pay attention to. It shows that the “stress” part is in fact separate sleep. A safe parent can trump many unsafe situations stressful situations (both in the bed, and in a crib ie. the recommended room sharing). SIDS IS defined as an unexplainable death. The separation IS the stress, and SIDS IS the result. The explanation of a co-sleeping death falls on the parent’s mistakes. The mistakes are defined and preventable. Why will you not talk about unexplainable deaths that happen when a child sleeps alone in a crib? WHY? And one more “WHY?” (just for emphasis) If you are concerned with untimely child death, why would you not pay any attention to the connection between separate sleep and accurately diagnosed SIDS? I have an opinion on that as well.
Maybe it’s because you do not believe that sleeping next to your child was the right thing for you, and that you are now justifying your decision with anti-co-sleeping rhetoric. I do understand that.
The hatred for AP attitudes must come from somewhere. It all seems juvenile to me, I’m done with this blog!
Hugh: There are many things doctors and scientists give advice on that they have not actually done. Again, you come out with the you must nor have done this or you would understand. Not scientific, Hugh.
Again, please look at your own issues regarding this and why does her discussing something that she has not done and would not do bother you do much? Should male doctors never be allowed to discuss breastfeeding and lactation? Of course, they have never done this. Please develop better discussion skills for the sake of those reading these posts. If a parent hadn’t spanked their child should they be allow to discuss spanking? Would you assume anyone who disagreed with this practice was “justifying” not spanking their child? Bad logic and another childish attempt to attack the blogger.
I have seen many blogs and posts where APers accuse others of disagreeing because they are embarassed about their own parenting methods. I imagine this line of reasoning comes fromo projecting their own defensiveness regarding their parenting on to others who have made different choices. Hugh – Possibly you yourself are justifying your own choices? It seems very likely to me.
Here we are discussing a study. Do you disagree with the study or just the fact that you don’t like that it is being discussed? Do you have an opinion about the study? Do you have any research to back up opinions?
Yeah – “honest injun” – is the best you could do? Possibly, you are not aware of the intent to show the childishness in the response and no, no mature adult would read racism in to that comment. Possibly you yourself are justifying your own bad cosleeping habits or are just justifyinf choosing cosleeping.
apologies for the lack of spell check above 🙂
Hugh, you really doth protest too much. If you have any science that’s contrary to my supposed “spin”, I’ve already asked you to provide it. A list of parents who really, really like bedsharing and have been convinced by unreliable publications and websites that it protects against SIDS is not scientific proof of anything but the gullibility of those parents. There is no science that shows separate sleep is stressful to an infant, especially not one in a crib/bassinet right next to Mommy, and in fact, there is a study that claims the contrary (I’ve brought it up in an earlier post and procliamed my misgivings about it).
My decision not to sleep with my babies in bed (though I can’t say it never, ever happened – being but human) was based upon common sense – “instinct” if you will. Seems APers only credit instinct when someone’s “instinct” agrees with them. I happen to think many cosleepers decided to take up the practice on the basis of the false promises peddled by Sears, Tina Kimmel, McKenna and co.
Yes, some babies die in cribs. The point is, however, that proportionally, more young babies die in adult beds. Also, no amount of “safe” bedsharing can compensate for a small baby ,an exhausted mother, or the presence of bedclothes normally used in the western world.
Rachel – too bad you didn’t stick around with a more open mind. Maybe one day, when you’re older and wiser…
Hi.
Please forgive me if I’m posting this in the wrong area (Moderator, feel free to move it if you wish)…..
I’m desperately trying to find results of any studies on whether overnight monitoring of oxygen saturation can prevent (or even reduce risk of ) SIDS.
I have found posts saying that the studies have been carried out (possibly in the UK?) but can’t find any results. I can find hundreds of quotes that apnea monitors don’t prevent SIDS, but I’m talking about oximeters.
Any help greatly appreciated,
Alan (parent of prem twins)
Alan,
I did a Medline search and can’t find any such studies, either. I’ll try and keep looking though.
Do your twins go to a premie clinic for follow up? Perhaps the doctors there would know.
Hi Estherar
I did mention it to our consultant when he sent our daughter home on oxygen, but without an oximeter. I queried not having an oximeter to take home with us, but all he said was that he wouldn’t be sending her home after all the input from the doctors and nurses if he thought she wouldn’t be OK. But on reflection, I think he probably meant that she was at “no greater risk than any other baby”. (For our peace of mind, I purchased my own oximeter).
He said that he wasn’t aware of any such research. However, I have a lot of respect for him, and he said that if having an oximeter for a year would prevent all cot deaths, every parent would have one. (He didn’t mention costs, but I guess that if thousands were sold to parents, the price would come down from the current £800 , or that someone would set up a scheme where parents could rent one for 1 year).
But my theory is that an alarming oximeter (like our daughter had for the entire time she was in hospital) WOULD prevent cot-deaths, as they would give an early warning – probably within 2 minutes of a potential problem. Maybe not ALL, but I understand that the genuinely unexplained deaths are linked with a lack of oxygen in some way. You see, I suspect that in NICU wards, they don’t have unexplained cot-deaths!
The lady I spoke to FSID (The Foundation for the Study of Infant Deaths) in the UK were also not aware of any such research. Maybe I should contact one of the big London hospitals?