








In mid 2006, a new vaccine against 4 strains of Human Papilloma Virus (HPV) was approved by the FDA for use in girls and women aged 9-26 years of age. Named Gardasil, it has been shown to effectively prevent acquisition of the strains of HPV that cause some 70% of cervical cancer cases and 90% of genital warts. Before being approved, the vaccine was tested on over 21,000 females and shown to be safe and extremely (99-100% depending on virus strain) effective – so much so, that the clinical trials were terminated early on the grounds that it was not ethical to deny the vaccine to the group receiving the placebo. Many US states have since implemented (or are in the midst of implementing) programs to routinely give the vaccine to girls entering the sixth grade.
It is certainly legitimate to debate whether this vaccine should be one routinely given to girls so young, if the vaccine’s effects will last into young adulthood for those given it as little girls (so far we know the effects last at least 5 years), and whether the girls will interpret having gotten the vaccine as carte blanche to have sex – unsafe or otherwise. But the attacks on the vaccine, both from the far right and the usual anti-vax contingent, have been to portray the vaccine as dangerous to the point of deadly: “Death toll from vaccine rises”, cries one such headline. And as to be expected, the personal injury lawyers are girding their loins.
The claims of death from the result of vaccination with Gardasil are based upon reports submitted to VAERS. As of late October, over 10,000 reports of adverse reactions (most of them – 94%, to be precise – minor) have been reported for Gardasil, among them 27 reports of deaths following receipt of the vaccine – this after about 20 million doses of vaccine have been given. However, as VAERS itself takes pains to point out:
When evaluating data from VAERS, it is important to note that for any reported event, no cause and effect relationship has been established. VAERS is interested in all potential associations between vaccines and adverse events. Therefore, VAERS collects data on any adverse event following vaccination, be it coincidental or truly caused by a vaccine. The report of an adverse event to VAERS is not documentation that a vaccine caused the event.
It’s important to note that deaths among the participants of the Gardasil trials were also noted, but when you see the breakdown of the causes of death, it’s fairly obvious that none of them had any clear connection to the vaccine (emphasis mine):
Across the clinical studies, 17 deaths were reported in 21,464 male and female subjects. The events reported were consistent with events expected in healthy adolescent and adult populations. The most common cause of death was motor vehicle accident (4 subjects who received GARDASIL and 3 placebo subjects), followed by overdose/suicide (1 subject who received GARDASIL and 2 subjects who received placebo), and pulmonary embolus/deep vein thrombosis (1 subject who received GARDASIL and 1 placebo subject). In addition, there were 2 cases of sepsis, 1 case of pancreatic cancer, and 1 case of arrhythmia in the group that received GARDASIL, and 1 case of asphyxia in the placebo group.
Luckily for us, the VAERS has a searchable database, so we can search for the deaths reported after Gardasil administration. If the cause of death were really the vaccine, we would expect the deaths to be grouped within a certain (short) time period after administration and manifest in similar manners.
Here are the results of my VAERS database search for deaths associated with Gardasil. As you can see, I’ve managed to find 20 cases out of the 27 reported as of late August. The deaths are at variable times after administration of the vaccine. after different numbers of vaccine doses, and of what seem to be variable causes. This is consistent with the CDC’s assessment of the deaths, and why it considers them almost certainly not the result of the vaccine:
As of August 31, 2008, there have been 27 U.S. reports of death among females who have received the vaccine. There was no common pattern to the deaths that would suggest that they were caused by the vaccine. Of the 27 U.S. reports:
* 3 reports were related to diabetes or heart failure
* 3 reports were related to viral illnesses or meningitis (an infection in the brain)
* 2 reports were related to drug use
* 2 reports were related to blood clots
* 5 reports are being evaluated (attempting to follow up/identify case)
* 1 report is still under review or VAERS is still waiting for additional medical records, such as an autopsy report or death certificate
* 1 report of seizure disorder (history of seizures)
* 3 reports had an unknown cause of death
* 7 reports that could not be evaluated because they did not have enough information to identify the person, or to verify that a person had died.
According to the National Center for Health Statistics, the death rates for young women in 2005 (the latest year available) were:
10-14 years: 14.4/100,000 population
15-19: 37.2/100,000
20-14: 48.2/100,000
25-29: 54.4/100,000.
27 deaths out of 20 million doses Gardasil given (which translates at the very least to over 6 million girls) falls well within the expected death rates from any cause. Some of those deaths, unfortunately, will fall into the time period following a vaccine. Ditto for any other adverse reaction that may happen.
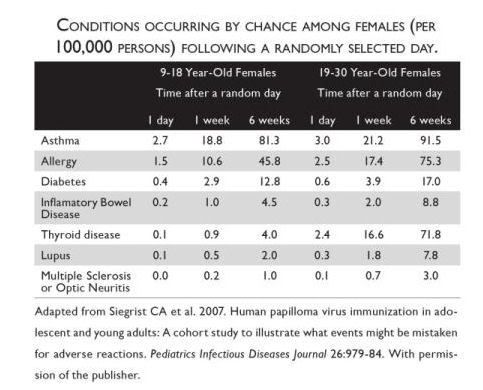
In fact, Siegrist et al tried to pre-empt this line of thinking by checking the incidence rate of various adverse events in a female population that happened at various time points after a given day, chosen arbitrarily. It’s a pity they didn’t look at death as an adverse event as well, but the results, as shown in the table below (courtesy of a book I’ve already recommended, Do Vaccines Cause That?), are pretty startling (click on the table to see it full-size):
In the interest of full disclosure: unless there are any unexpected revelations about Gardasil in the next four years, I intend to give it to my daughter when she comes of age – even though she’s going to an all-girls school. (She does have a boyfriend, however. And they play ‘getting married’ very often. Sometimes she wears the white dress, sometimes he does 🙂 . ).
 :
:  :
:  :
:  :
:  :
:  :
:  :
:  :
:  :
:  :
:  :
: 
Filed under: Risk perception, Vaccines |

My suspicions were aroused when it became apparent that it was the DRUG REPS who were pushing the vaccine rather than most of the doctors I know. Gardasil is made by Merck, which needs a new cash cow badly because of the sums it’s paying out for Vioxx claims.
Further, nearly all the women who ask me for advice [mothers of girls going into the army, here in Israel, for the most part], are unaware that so far we only know that it protects for 5 years, and that it doesn’t protect against 100% of all HPV strains. Even in our subsidized system, the three injections are very expensive, which also comes as a shock. And lastly, that yearly Pap smears are still needed.
One of the doctors I work with counsels that the best preventative is still a box of condoms, which protects against ALL STDs, HPV, and pregnancy as well, and it’s a heck of a lot cheaper.
What have you to say to the reports of Guillain-Barre Syndrome which have been associated with Gardasil, btw?
That’s really interesting. I’d read the articles about how dangerous Gardasil was, and hadn’t seen anything calling it safe until now. I love that most of the deaths were from car accidents… How anyone can include those numbers in the statistics is beyond me. (I understand why VAERS does, I’m referring to those who write articles about it.)
My daughter is only 8 months old, so I have a while to decide whether or not I want her to get the vaccine. I chose not to get it myself, because my husband and I both abstained before marriage, so it seemed rather pointless. Part of me doesn’t want her to get it, because I’d like her to make the same choices I did. However, the other part of me wants to protect her in any way I can, just in case.
Antigonos,
In the initial stages of a drug/vax being introduced, reps are going to push whatever they’re pushing far more than doctors because they have a financial interest in doing so. Doctors tend to be more cautious and (at least here) less financially involved. This has nothing to do with how good the product is, IME. various new pediatric vaxes seem to be undergoing the same wary acceptance.
Mind you, I first received a real education about the vax not from a drug rep, but via a lecture at a conference about new vaxes being incorporated into the Israeli system given by Dr. Shmuel Rishpon (from the Health Ministry in Haifa). He mentioned HPV vaccine would be routine here around 2011 anyway – and I imagine the OBs and epidemiologists who crunched those numbers are no drug-rep patsies.
Anyway, as I said in the post, there is certainly room for debate about whether it’s a worhtwhile endeavor to vaccinate the whole of the female population against HPV (especially in a country like ours, where the cervical cancer rates are so low that the screening program is slightly different than in other countries). Telling the public that women have died from the vaccine? Not true nor kosher to allege.
I’m not impressed with GBS being associated with Gardasil either – apparently, the GBS, if at all vaccine-related – and there is some doubt about that as well – seems more likely to result from concurrent Menactra (meningococcal vaccine) vaccination.
curious… why are rates of cervical cancer lower in israel? because of the large orthodox population?
Most probably for genetic reasons (at least among the Jewish population).
An interesting and layperson-accessible article on the subject .
Wow this vaccine even causes car accidents!!!!!! What a powerful vaccine!!!!! (Kidding). Amazing how some folks can mangle the truth.
I just read the article. It seems to dismiss keeping niddah since it is only kept by a minority. My understanding is tha about 25-30% of the population is orthodox. Why do they dismiss that as too low to affect the results?
I’m not sure why niddah would prevent HPV acquisition in the first place. Apparently, the time of the month in which you have sex has no bearing upon catching HPV.
not niddah per se, but, on average, people who keep niddah do not have multiple sex partners.
There may be a correlation, though not all women who currently keep niddah were virgins on their wedding night (and incidentally, I’m always amazed at some of the women I meet at the Mikveh…who are not religious AT ALL, but still see fit to keep this mitzvah. Kol Hakavod to them!).
Thanks for doing your research on Gardasil. I know one of those “evil drug reps” that sells it and get really tired of ignorant people who do nothing more then read a hype news story and just assume that it’s all true.
As for GBS, the CDC does address this issue in their adverse event reports. Basically there are fewer cases of GBS in a vaccinated population then they would expect to see by chance in a non-vaccinated population.
By the way,,,, not only does it prevent cancer,,, think about Leeps and what that procedure does to the cervix. Each time a patient has a procedure done it reduces their chance of being able to carry a pregnancy to full term.
One of the doctors I work with counsels that the best preventative is still a box of condoms, which protects against ALL STDs, HPV, and pregnancy as well, and it’s a heck of a lot cheaper.
Condoms, while reducing the chances of HPV transmission, are by no means 100% effective in preventing HPV infection. Additionally, HPV can be transmitted through oral contact (I mean kissing…get your minds out of the gutters, people!) and is associated with head and neck cancers as well as cervical, anal, and possibly skin cancers. So really boys ought to be vaccinated as well.
Ireland just eliminated the vaccine for women because it cost too much (10 million euro…really not that much of their budget). They also don’t do paps until age 25.
Of course if you have money, you can have access to both of them. Nice. It scares me that women’s health is so easily disregarded and even more so in poorer communities.
As a nurse and NP that has worked with adolescents, I was happy to hear about the vaccine but a little concerned that the marketing would provide another story I would hear as to why they weren’t using condoms.
Great blog BTW!!
Thanks Debbie!
I would really hope the vaccine wouldn’t provide an excuse not to use condoms. Then again, I’ve never heard HPV as an excuse for people to use condoms in the first place (see the previous and pertinent comment by Dianne). Usually people are more afraid of HIV, chlamydia, gonorrhea and syphillis…
I got the shot in Novembber 2007. In Feburary i started vomiting daily, had high blood pressue, kidney issues, abdominal pain, headaches, was blacking out and many more symptoms. I was in and out of the hospital for about 3 months. I still to this day suffer the side effects of this horrible shot. Luckily I was one of the lucky few that found help right away. Though the medical doctors told me I was faking I started finding answers from a nutritionalist in Califronia. He has helped me get a lot better. If any mothers read this and need advice on how to help their daughter please email me at lyrics4christ@gmail.com or my mother at jonesfam123@cox.net. If you dont need to get the shot dont…. it is not worth the risk. at least do the research before coming to your desicion.
Four months after you received the dose you developed these symptoms. Sorry to break this to you but it wasn’t the vaccine. The first week, first two weeks, maybe but not 4 months later. The nutritionist from California is a crack pot.